
It is a Wednesday morning and I’ve made my usual trek to UCSF for our weekly Renal Grand Rounds. A drive to the BART train station. From BART to MUNI where I pick up the N-Judah bus, which drops me off in front of the medical center about 45 minutes after I’ve left my home. I take my usual perch in the back of the room so in case I get bored, my email checking and Sudoku playing on my iPhone will be as inconspicuous as possible. This week’s speaker is Dr. W, a transplant nephrologist from the East Coast. He is an attractive Asian man of about my height, age, and weight with a pleasant smile and easy demeanor.
His first PowerPoint slide reads: “Trying to Increase Live Donor Kidney Transplant: Dreaming the Impossible Dream?” He starts off reviewing the state of kidney transplantation in this country. The list of people with end-stage kidney disease waiting for a kidney transplant grows each year. The number of kidneys from the dead is not nearly enough. Many on the wait list die waiting for a kidney. The number of kidneys from the living has been fairly stagnant. How can we get more of the living to donate, he poses?
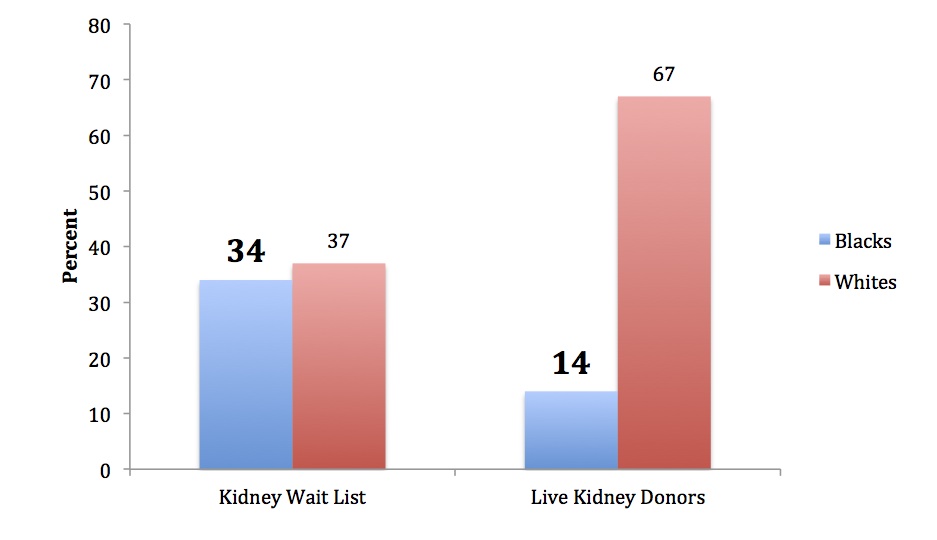
Then there it was—racial disparities. Whites make up a little over a third of the waitlist but donate more than two-thirds of the live donor kidneys, while blacks make up a third of the waitlist but only donate 14% of the live donor kidneys. A large bar graph projected onto the screen, providing a clear visual image of the disparity.
post1
He let the words hang in the air and looked to the floor for a moment, allowing us, the audience of nephrology fellows, general nephrologists, transplant nephrologists, and transplant support staff to speculate silently about why this huge racial disparity may be. Why blacks aren't doing their share.
A burn sprays through the pit of my stomach and my heartbeat quickens and my body stiffens as they always do when things about black people come up in these type of lectures, whether it be at UCSF, San Francisco General Hospital, or the national kidney conferences. Because when black people come up in these lectures...it ain’t never for something good.
I feel the heat of an imagined spotlight shining directly on me. I feel sideways glances upon me. Even eyes peeking out from the backs of the heads in front of me.
I am the only black physician within the Division of Nephrology at UCSF now or in the last 15 years. That's including San Francisco General Hospital and the VA. I am always keenly aware of this, of being the only one.
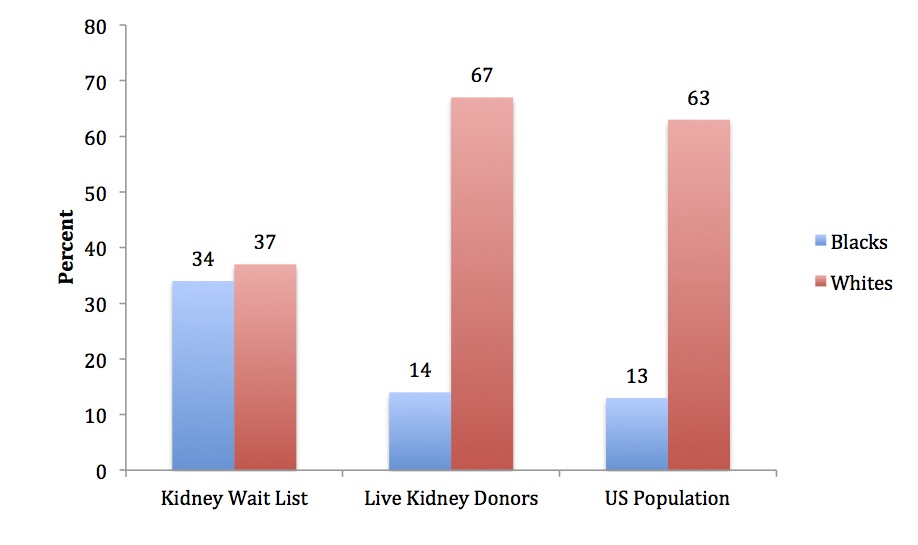
I want to raise my hand and interrupt Dr. W’s talk to ask—“Given that blacks only make up 13% of the population in this country, but develop end-stage kidney disease four times as often as whites, and medical reasons are most often why potential donors are excluded, and the most common causes of kidney failure run in families…what do you think a reasonable goal for living donation from blacks would be?” An impressionable audience should be given the full picture of a thing, not just the frayed corner that makes the point you want to make. Everyone should question how blacks could be expected to donate kidneys beyond their numbers in the population—especially when they are likely to be related to someone who is sick, often as a result of high blood pressure and diabetes which cause two-thirds of kidney disease in this country and tend to run in families. Everyone should question why the data are being shown by race anyway when donor and recipient don’t have to be the same race. But I imagine I am the only one thinking such questions.
I hesitated. I needed to take in some slow deep breaths first to slow down my pulse, relax my shoulders, and soothe my quivering insides in order to remove any traces of emotion from my voice and body language. I wanted to come across matter-of-factly and dispassionate, not the Angry Black Woman I risk being labeled every time I open my mouth to say something about race in these rooms.
Later, he brought up the racial disparity again. Showed his bar graph again. Still I hesitated. My deep breaths aren’t working. I decide to wait until the end of the lecture, when questions from the audience are welcome. Less confrontational. I rehearse my question in my head, visualizing my posture relaxed and my tone calm.
His talk ran long. The senior transplant nephrologist jumped in with his question, whose answer prompted his follow-up question. Something about if transplant programs with more money have higher live donation rates than less wealthy programs.
Only time for one more question. My right hand will not unclench itself from the left one in my lap to raise quickly enough. Another transplant nephrologist raised her hand to ask something about donor survival.
Opportunity missed. I failed to speak up. And because I didn’t speak up, everyone was filing out of the room with Dr. W’s frayed corner of a picture emblazoned in their minds. It is hard being the only one always speaking up; to be so bold time and time again; to always be thought of as Angry—never Informed or Concerned or Passionate.
I approached Dr. W at the dais to ask my question.
“And who are you?” he asked pleasantly before I could start.
“Oh, I am one of the general nephrologists based at our San Francisco General Hospital. And I also happen to be a kidney donor,” I smiled.
I deliver my question as rehearsed. Less confrontational. “What do you think would be a reasonable goal for living donation from blacks—given that blacks only make up 13% of the population in this country, but develop end-stage kidney disease four times as often as whites, and medical reasons are most often why potential donors are excluded?”
He looked away, surprised or taken aback I couldn’t tell.
“Well,” he eventually mustered, “each person on the waitlist only needs one donor.”
“Yes, but,” I asked, “given that the diseases that are causing kidney failure run in families…”
He couldn’t find any new words to muster.
Maybe I didn’t fail completely. Maybe he will present the whole picture next time.
post2